
Nutritional Recommendations for Patients with Inflammatory Bowel Disease
1. Introduction
Ulcerative Colitis (UC) and Crohn’s Disease (CD), collectively known as Inflammatory Bowel Disease (IBD), is a progressive and unpredictable chronic disease that mostly affects but not limited to the colon. This disease is known to cause inflammation and dysregulation in the gut causing multiple nutrition related problems but also affecting quality of life for patients and families. (Mahan & Raymond, 2017)
Conventionally IBD was considered a disease of western countries (with a more Western diet) however, studies now show that there is a rise of IBD in eastern countries (eastern Europe, Asia, and South America) and a plateau in western countries (Europe, Oceania, and North America). IBD increases where countries are becoming more industrialised with more socioeconomic growth. UC have a higher prevalence than CD in European and Asian countries and data is limited for sub-Saharan Africa. (Mak, et al., 2020)
The cause of IBD is not fully understood, but research suggests that immune system dysregulation, genetics, environmental factors, diet, and the gut microbiome may all contribute. Diet has a significant impact on the gut microbiome, and adopting a more Western diet can have negative effects. The changing prevalence of IBD in eastern countries suggests that environmental factors, including diet and food quality, may play a larger role than genetics (Hammer & Langholz, 2020).
2. Background
UC is characterised by continuous inflammation in a specific part of the colon, starting from the rectum and spreading upwards. It can be effectively treated with a colectomy. The damage caused by UC primarily affects the mucosal and submucosal layers of the colon.
CD is considered more severe than UC. It can occur anywhere in the digestive tract, with healthy non-inflamed areas in between the inflamed parts. CD affects all layers of the gut, resulting in a distinctive cobblestone appearance. Complications of CD include strictures and fistulas in the gut. (Mahan & Raymond, 2017)
Common symptoms of IBD include diarrhea, bloody stools, urgency to empty bowels, abdominal pain, bloating, poor appetite, fatigue, nausea, and vomiting. Diarrhea can lead to complications such as nutrient deficiencies, dehydration, weight loss, fatigue, and social anxiety related to eating in front of others. (Morton, et al., 2020)
3. Nutritional challenges
When considering the clinical challenges of IBD, it is crucial to examine the impact of Food Related Quality of Life (FRQoL). Many individuals, particularly children and teenagers who are newly diagnosed, develop a fear of eating to avoid flare-ups or discomfort. This often leads to the elimination of entire food groups, resulting in a deficiency of essential macronutrients and micronutrients. (Whelan, et al., 2021)
One of the major challenges in IBD is nutrient absorption, particularly during flare-ups. Amino acids, fatty acids, carbohydrates, vitamins, and minerals are primarily absorbed in the jejunum and ileum. During flare-ups, these nutrients can be lost, leading to potential complications. If the ileum is more affected, there is a risk of developing deficiencies in fat-soluble vitamins (A, D, E, K, and B12). Individuals with CD are more likely to be negatively affected, as CD can impact the small intestine. However, people with UC, which affects the larger intestine, can still develop deficiencies due to diarrhea rather than malabsorption. Micronutrient malabsorption in IBD can lead to decreased bone mineral density, primarily caused by inadequate intake of calcium (often due to avoiding dairy out of fear), poor absorption of calcium (due to diarrhea, nausea, vomiting, or medication use), vitamin D deficiency, decreased physical activity (due to fatigue or pain), and inflammation (Foundation, 2023).
Children with IBD may experience growth problems due to malabsorption and increased nutrient needs. These increased needs arise from complications such as diarrhea, use of certain medications (especially corticosteroids), lack of appetite, micronutrient deficiencies, malabsorption, and infections. Children with IBD who experience pain, nausea, and vomiting are likely to have reduced appetite, further hindering their growth. In severe cases, enteral or parenteral feeding may be necessary. (Balestrieri, et al., 2020)
These complications are interconnected and can exacerbate one another. Treating one complication may have a positive impact on the others.
Recommendations for nutrition
There is no one-size-fits-all diet for IBD, so dietary recommendations need to be personalised for each patient based on their specific needs and triggers. Factors such as symptoms (remission or flare-up), type of IBD (UC or CD) and its location, presence of strictures, medications, and complications (such as nutrient deficiencies or growth failure) should be taken into consideration when designing a diet plan.
A Western diet, which is high in saturated and trans fats, red meat, and refined carbohydrates, while low in fruits, vegetables, and fibre, has been shown to negatively impact the gut microbiota. The gut microbiota plays a crucial role in gut health and the onset and remission of IBD. Restoring the gut microbiota through dietary changes can potentially improve periods of remission (Balestrieri, et al., 2020).
The International Organisation for the Study of Inflammatory Bowel Diseases (IOIBD) has developed a set of guidelines based on the best current evidence to manage IBD. It provides guidance for health professionals and patients regarding which foods maybe harmful, beneficial, or safe to consume. The recommendations are focused on dietary patterns to control and prevent relapse of IBD. The recommendations are made in terms of specific food types:
- Fruits and Vegetables: It is recommended for CD patients to consume a moderate to high amount of fruits and vegetables. However, in cases of symptomatic fibrostricturing disease, it is advised to restrict intake of insoluble fibre. Soluble fibres found in certain fruits and vegetables can benefit the gut microbiota in individuals with CD.
- Refined Sugars and Carbohydrates: There is insufficient evidence to recommend specific changes in complex carbohydrates, refined sugars, or fructose intake for CD and UC patients. However, a low FODMAP diet might be considered for those with persistent symptoms despite inflammation resolution. Evidence supporting this recommendation is limited.
- Wheat and Gluten: There's limited evidence supporting the restriction or avoidance of wheat and gluten in UC and CD. Gluten restriction may offer benefits, possibly due to reduced FODMAP intake. Some dietary components, such as emulsifiers and thickeners, may need limitation, but evidence supporting these recommendations is very low.
- Red Meat, Processed Meat, Poultry, and Eggs: Moderate consumption of unprocessed red meat, lean chicken meat, and eggs is considered safe for CD patients, while reducing red and processed meat intake is advised for UC patients. High animal protein intake is linked to an increased risk of IBD.
- Dairy: Consensus was not reached for the consumption of pasteurised dairy products in CD or UC patients, but unpasteurised dairy products should be avoided. Lactose intolerance is more common in individuals with CD and UC, and there is no clear evidence supporting the benefits of eliminating dairy in patients with UC. Dairy composition varies, including lactose and additives like emulsifiers and thickeners. Lactase deficiency is more common in individuals with CD and UC, and baseline dairy intake doesn't appear to affect disease flares. Unpasteurised milk should be avoided due to infection risks.
- Fat: In CD, it's advisable to reduce saturated- and trans-fats. In UC, myristic acid consumption should be reduced. Omega-3 fatty acids from marine fish are beneficial. In UC, increased meat and total fat intake are associated with a higher risk of relapse.
- Alcohol: The impact of alcohol on IBD is inconclusive. While it may induce flares, a daily glass of red wine can reduce faecal calprotectin. The relationship between alcohol and IBD remains complex and warrants further research.
- Maltodextrin and Artificial Sweeteners: Limiting intake of maltodextrin-containing foods and artificial sweeteners is recommended for both CD and UC patients, despite the low level of evidence supporting this.
- Emulsifiers and Thickeners: Consumption of processed foods containing carrageenan, carboxymethylcellulose, and polysorbate-80 should be reduced, even though evidence supporting this recommendation is very low.
- Nano-particles and Sulphites: Limit exposure to processed foods containing titanium dioxide and sulphites, as their effects on IBD are not fully understood. More research is needed to establish dietary recommendations in this regard.
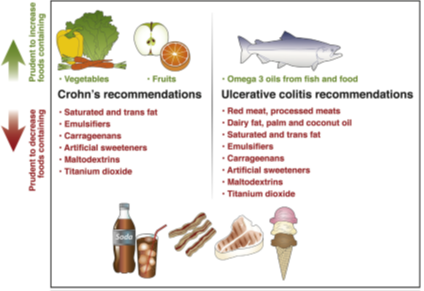
Furthermore, for IBD management, a low FODMAP or lactose-free diet might help alleviate symptoms. The Mediterranean diet is considered safe for patients without allergies or food intolerances. Prebiotics and probiotics are also under study to restore the gut microbiome, but further research is needed to understand their optimal use.
The picture below gives a summarised representation of what should be done regarding diet. (Levine, et al., 2020)
4. Conclusion
IBD poses significant challenges to patients' health and well-being, affecting both adults and children globally. While the Westernisation of diets has been linked to the rise of IBD, recent data suggest a similar trend in eastern countries undergoing industrialisation. Nutritional management plays a vital role in ameliorating the impact of IBD, particularly in children, where the fear of eating and malabsorption present significant hurdles. A personalised approach, considering disease type, location, and individual triggers, is crucial in formulating effective dietary recommendations.
Recommendations such as limiting certain food groups, considering fat sources, alcohol intake, and the use of additives, can contribute to better management of IBD symptoms. The role of specific diets such as the Mediterranean diet and the manipulation of gut microbiota through prebiotics and probiotics require further investigation for optimal integration into the management of IBD. The emerging guidelines from the International IOIBD serve as a foundation for clinicians and patients in navigating the complex interplay between diet and IBD, aiming to improve overall patient outcomes and quality of life.
References
Balestrieri, P., Ribolsi, M., Guarino, M. P. L. & Emerenziani, S., 2020. Nutritional Aspects in Inflammatory Bowel Diseases. Nutrients, 12(372).
Foundation, C. a. C., 2023. Crohn's and Colitis Foundation. [Online]
Available at: crohnscolitisfoundation.org
[Accessed January 2017].
Godala, M., Gaszynska, E., Zatorski, H. & Maleca-Wojiciesko, E., 2022. Dietary Interventions in Inflammatory Bowel Disease. Nutrients, 14(20).
Hammer, T. & Langholz, E., 2020. The epidemiology of inflammatory bowel disease: balance between East and West? A narrative review. Digestive Medicine Research, 3(48).
Levine, A. et al., 2020. Dietary Guidance From the International Organisation for the Study of Inflammatory Bowel Diseases. Clinical Gastroenterology and Hepatology, 18(6), pp. 1381-1392.
Mahan, L. K. & Raymond, J. L., 2017. Krause's Food & The Nutrition Care Proses. 14 ed. St. Louis, Missouri: Elsevier Inc..
Mak, W. Y., Zhao, M., Ng, S. C. & Burisch, J., 2020. The epidemiology of inflammatory bowel disease: East meets West. Journal of Gastroenterology and Hepatology, Volume 35, pp. 380-389.
Morton, H., Pedley, K. C., Stewart, R. J. & Coad, J., 2020. Inflammatory Bowel Disease: Are Symptoms and Diet Linked?. Nutrients, 12(10), p. 2975.
Whelan, K., Murrells, T., Myfanwy, M. & Fraser, C., 2021. Food-related quality of life is impaired in inflammatory bowel disease and associated with reduced intake of key nutrients. American Journal of Clinical Nutrition, Volume 113, pp. 832-844.
If you liked this post you may also like



