
Cow’s Milk Protein Allergy
Food allergy is a global burden. It is estimated that approximately 220-520 million people across the world suffer from food allergy, with incidences estimated to be greater in toddlers (5-8%) than in adults (1-2%).
In South Africa, it is estimated that approximately 2.5% of children suffer from food allergies. Preliminary data from the South African Food Sensitisation and Food Allergy (SAFFA) study has demonstrated a prevalence of Skin Prick Testing (SPT) ≥1 mm to any food of 11.6%, SPT ≥3 mm of 9.9% and SPT ≥7 mm of 4.2%. Challenge-proven food allergy prevalence is 1.8%, egg allergy 1.4% and peanut allergy 1.1%. Cow’s milk protein allergy (CMPA) peaks in infancy with a prevalence of 2-3% of the infant population.
Nutritional management of Cow’s Milk Protein Allergy (CMPA)
Breastfeeding should always be the first option in preventing CMPA. Mothers of infants with CMPA who are breastfeeding should be supported and encouraged to continue breastfeeding. However, for those mothers who cannot breastfeed, a clinically proven breast milk substitute is recommended for the prevention of the allergy. Certain partially hydrolysed whey infant formulas and extensively hydrolysed casein formulae have proven to be effective in reducing the occurrence of eczema or CMPA in high-risk individuals. It is thus recommended to utilise these formulae for infants with a family history of allergy.
The recommended food for the dietary management of mild or moderate CMPA in infants who are not breastfed is an extensively hydrolysed infant formula. The recommended formula for the dietary management of non-breastfed infants with severe CMPA is an amino-acid based formula. However, amino acid formula comes at a cost and thus the South African Food Allergy Working Group (SAFAWG) recommends amino acid formula only in these circumstances:
- infants with CMPA with severe or life-threatening symptoms
- patients with ongoing symptoms on an extensively hydrolysed formula
- infants with severe growth faltering
- in rare circumstances where a stringent exclusion diet in the breastfeeding mother has failed to resolve symptoms in the infant
Other mammalian milks and plant-based milks are not routinely recommended for management of CMPA.
Please refer to Figure 1 below for an algorithm regarding nutritional management of CMPA.
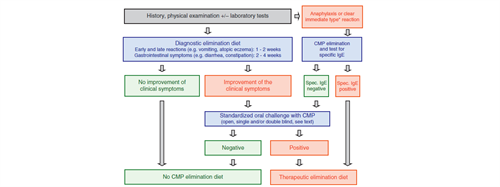
Figure 1: Algorithm for infants and children with symptoms suggestive of cow’s-milk protein allergy (CMPA). eHF: extensively hydrolysed formula based on cow’s-milk protein, AAF: amino acid–based formula. (Credit: ESPGHAN, 2012)
Conclusion
Cow’s milk protein allergy is the most common manifestation of food allergy in infants. Nutritional management of this condition requires risk assessment and nutritional intervention measures in order to ensure that particular nutritional requirements are met that promote normal growth and development of the infants for whom they are intended.
Fiochi et al. World Allergy Organization (WAO) Diagnosis and Rationale for Action against Cow's Milk Allergy (DRACMA) Guidelines. 2010. Pediatric Allergy and Immunology, 21(s21):
1–125.
Ibid.
Levin et al. South African food allergy consensus document 2014. 2015. SAMJ, 105(1): 62-65.
Ibid.
Koletzo et al. Diagnostic Approach and Management of Cow’s-Milk Protein Allergy in Infants and Children: ESPGHAN GI Committee Practical Guidelines. 2012. JPGN, 2: 221-229.
Ibid.
If you liked this post you may also like



