
Lactose Intolerance and Cow’s Milk Allergy
With an aim to raise awareness in this National Asthma and Allergy Awareness Month (May), the NNIA investigates the relationship between allergies related to lactose intolerance (LI) and cow’s milk allergy (CMA).
These are frequently misdiagnosed and poorly treated, as the symptoms of both conditions are very similar. The reaction from both LI and CMA is from the same source, milk, but are caused by different factors in the milk and mechanisms within the human body.1 The treatment for these two conditions is distinctly different – unnecessary milk restrictions and the reactions that occur due to misdiagnosis could have health implications on the patient.1
Milk contains essential nutrients, including calcium, magnesium, selenium, riboflavin, vitamin B12, as well as pantothenic acid. It is also a key source of dietary energy through its high-quality proteins and fats.4 Milk and milk products have been associated with a reduced risk in chronic diseases and conditions such as hypertension, cardiovascular disease, metabolic syndrome, type 2 Diabetes, as well as osteoporosis.5 Unnecessary dietary restrictions are not recommended given the stated health benefits.
It is therefore important for healthcare professionals to provide patients with factual information on the difference between LI and CMA, allowing patients to implement the correct management approach to address their illnesses. This is especially vital in developing countries where individuals typically do not have access or the financial means to seek medical expertise.
Lactose intolerance
Lactose intolerance is one of the most common food intolerances and, in a paediatric context, it is the most common carbohydrate intolerance. Essentially lactose intolerance is a deficiency in lactase, an essential enzyme that is necessary to break down lactose, a sugar found in milk or milk products, in order for it to be digested.1,2 When lactose is undigested, it becomes fermented by gut microbiota; abdominal fluids are driven to the gut lumen via osmotic force or fatty acids and gasses are produced. This causes abdominal pain, flatulence, nausea, bloating and diarrhoea. Symptoms are typically evident after 30 minutes to two hours after consuming lactose related foods.1
Types of lactose intolerance 1:
- Congenital lactase deficiency:
A rare recessive autosomal disease determined by little to no enzymatic activity from birth. Leading symptoms include diarrhoea, intestinal meteorism and malnutrition, especially during the first days of life due to lactation of breast milk or formula.
- Primary lactose intolerance or adult-type lactase deficiency:
A common recessive condition that arises due to regulated variation of the lactase gene through development. Patients primarily produce a substantial amount of lactase until it abruptly diminishes due to genetics. This is the most common type of LI (more that 50% of people in South Africa are lactase persistent). African children typically begin experiencing symptoms as early as 2 – 3 years old.
- Secondary lactase gene expression:
A secondary short-term condition that arises due to intestinal damage from diseases including infections, food allergies, celiac disease, small bowel bacterial growth, Crohn’s disease and enteritis from chemotherapy.
Cow’s Milk Allergy
Food allergies are triggered by proteins within the specific food. CMA is one of the most common food allergies, especially within the first years of life.1 Immunoglobulin E (IgE) mediated reactions (allergies caused by IgE antibodies)9 often take place within the first two hours of cow’s milk consumption, where non-IgE mediated reactions develop after two hours or days after consumption.1 Allergic reactions from milk protein are due to protein fractions in emulsion (caseins) or whey (milk albumin) and is type IV, mediated by T lymphocytes. Reactions lead to severe cell damage that triggers physical, mental and emotional reactions which vary in intensity and severity. 5
CMA is typically through the consumption of cow's milk but the consumption of milk from other animals such as sheep, goats, buffalo and other mammals also can cause the reaction.8
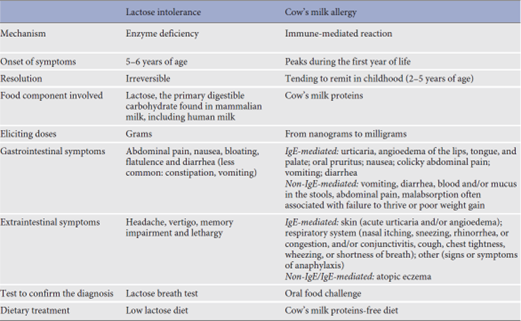
A Comparison
It is recommended for HCPs to make use of this easily printable and understandable summary1 of the main differences between LI and CMA for their daily practice and education to patients:
Generalised nutritional management tips for patients in developing countries:
Lactose Intolerance:
It is suggested that patients consume nutritional sources with a lower lactose level such as hard cheese, yogurt and lactose-hydrolysed milk products.1 Patients can also consume lactose-free milk (milk with added lactase) or consume fortified milks derived from soy, almond, coconut, oat, rice, cashew, macadamia, hemp or quinoa.6,7 It is also suggested that patients make use of supplements such as lactase and probiotics to induce colon microbiome adaption.10
The following nutritional recommendations are for those in developed countries who don’t necessarily have access to the above-mentioned substitutes or supplements:
A monitored lactose intake diet is recommended to manage LI.1 Research shows that adolescents and adults are able to tolerate up to 12 g or lactose in a single dose, equalling to about 1 glass of milk depending on its source.1,3 There is, however, no scientific evidence to determine how much lactose children can withstand without falling ill.1
For those in developing countries who generally have access to a range of fresh milk from livestock, it is recommended that patients consume goat’s milk as it has the least amount of lactose (4.2 g per 100g), followed by whole cow’s milk (4.5 g).1 Goat’s milk however lacks levels of folate and many vitamins such as B12, E, C and D.11 It is therefore suggested to supplement these or consume fortified milk as mentioned in the beginning of this section. It is also suggested that patients avoid buffalo and especially sheep milk as those sources are generally higher in fat and protein as well as lactose.1,4 Patients should also avoid skimmed and whole powdered milk as they are extremely high in lactose contents (50.5 g and 35.1 g).1
Other than milk, the following foods should be avoided1:
- Butter, whipped cream, yogurt, ice cream
- Cream cheeses, cottage cheese, soft cheeses (brie, ricotta), creamy or cheesy sauces
- Breaded or creamed fish and meat
- Baked goods or desserts that contain dairy
Cow’s Milk Allergy:
Even small amounts of protein in milk cause symptoms. Therefore, it is recommended that individuals avoid a diet that incorporates cow’s milk in any form.1
CMA is attributed to the early use and overuse in cow’s milk as a substitute for human milk in newborns and children.5 It is recommended to monitor and manage the intake of cow’s milk in this target group to prevent the development of CMA in infants and children.
Nestlé’s online tools and apps to manage LI and CMA
- Nestlé We Are Nutrition
This is a free tool on the AppStore that assists health care practitioners improve the nutrition of their patients through diagnostic and augmented tools. This platform additionally offers e-learning resources.
- Dietary Assessment Tools – Nutritools
Visit this website to view a list of tools which dietitians can use to manage a diverse range of patients.
- NutriLeap
This mobile friendly app for clinical dietitians calculates patient’s nutritional needs. This app additionally offers design functions for customised handouts and streamlines administration/documents.
- Nutricare Tools
Assess nutritional requirements for your patients and make use of this platform’s nutrition reference pages, meal plans and tips. Available on both AppStore and GooglePlay.
Conclusion
By communicating the above information and management tips to patients, health care practitioners can raise awareness for LI and CMA, as well as enable those who suffer from these conditions to improve their health and quality of life.
Reference list:
- Di Costanzo, M. and Canani, R.B., 2018. Lactose intolerance: common misunderstandings. Annals of Nutrition and Metabolism, 73(4), pp.30-37.
- Kretchmer, N., 1972. Lactose and lactase. Scientific American, 227(4), pp.70-79.
- Ratini, M. 2021. How much lactose can I tolerate? MedicineNet. https://www.medicinenet.com/how_much_lactose_can_i_tolerate/article.htm
- Food and Agriculture Organisation of the United Nations. s.a. Gateway to dairy production and products: milk composition. https://www.fao.org/dairy-production-products/products/milk-composition/en/#:~:text=Sheep%20milk%20has%20higher%20fat,from%20cows%2C%20buffaloes%20and%20goatsc
- Rangel, A.H.D.N., Sales, D.C., Urbano, S.A., Galvão Júnior, J.G.B., Andrade Neto, J.C.D. and Macedo, C.D.S., 2016. Lactose intolerance and cow's milk protein allergy. Food science and Technology, 36, pp.179-187.
- Link, R. 2018. What is lactose-free milk? https://www.healthline.com/nutrition/lactose-free-milk
- Coyle, D. 2018. The 9 best nondairy substitutes for milk. https://www.healthline.com/nutrition/best-milk-substitutes#TOC_TITLE_HDR_2
- MayoClinic. 2020. Milk allergy. https://www.mayoclinic.org/diseases-conditions/milk-allergy/symptoms-causes/syc-20375101
- The Royal Children’s Hospital Melbourne. 2016. Allergy and Immunology. https://www.rch.org.au/uploadedFiles/Main/Content/allergy/Non%20IgE%20Food%20Allergy.pdf
- Facioni, M. S., Raspini, B., Pivari, F., Dogliotti, E., & Cena, H. (2020). Nutritional management of lactose intolerance: the importance of diet and food labelling. Journal of translational medicine, 18(1), 260. https://doi.org/10.1186/s12967-020-02429-2
- Lima, M. J. R. et al., 2017, 'Nutritional and Health Profile of Goat Products: Focus on Health Benefits of Goat Milk', in S. Kukovics (ed.), Goat Science, IntechOpen, London. 10.5772/intechopen.70321.
If you liked this post you may also like

Access the Science, Insights, and Inspiration From NNIA's CNE 2026

How Human Milk Oligosaccharides Drive Neurodevelopment

