
World Obesity Day: Addressing Africa’s Sugar Problem

Reflecting on World Obesity Day (04 March), NNIA has investigated the high impact of obesity, mainly caused by high sugar consumption,1,2 to Non-communicable Diseases (NCDs) in sub-Saharan Africa and highlights how Healthcare Practitioners (HCPs) can facilitate the decrease in patient sugar consumption to address obesity, thus addressing NDCs in Africa.
Non-communicable diseases (NCD) are accountable for 15 million premature deaths annually, worldwide (85 % of these are recorded in low- and middle-income countries). It is expected that the number of NCD-related deaths will exceed the total number of deaths attributed to both HIV and tuberculosis in sub-Saharan Africa over the next 10 years.1,4 Obesity - a key contributor to NCDs such as diabetes, cardiovascular disease, cancer (colon and rectum) and chronic respiratory disease - is linked to high sugar consumption and is actively on the rise across sub-Saharan Africa. 1,2,5
The rise of obesity and its associated NCDs has been attributed to spatial, economic, and social factors that influence the physical activity and diet of communities. Where this is of particular concern is when these factors result in the consumption of poor-quality diets, and low levels of physical activity. 1 As countries develop, the differences between rich and poor become prominent through diet. People of poorer communities tend to adopt an obesogenic diet that comprises unhealthy dietary fat, sugars, and sodium as well as energy dense ultra-processed products. 5
It has been found that healthy foods are inaccessible and unaffordable in low-income and minority communities. The convenience stores in these communities primarily offer highly processed foods, candy, sugar-sweetened beverages (SSB), snacks with a high sodium level (which are also energy-dense); and lack healthy, fresh produce. 9 Research has illustrated an outstanding link between obesity and related NCDs with a high sugar consumption that is mostly due to the intake of SSBs. 1
In 2016, the World Health Organisation recommended that countries increase tax on SSBs, as a strategy to prevent and control obesity and NCDs. 1,2,3 South Africa was the first country in sub-Saharan Africa to announce the adoption of these taxes and successfully did so in 2018 by applying a tax rate of 11% on SSBs. 4 Although this tax did reduce the consumption of SSB, the total amount of sugar consumed through other sources (sugar compensation) and the consumption of table sugar, remained consistently high. It has been deemed that targeting individual components of diets (in the form of SSB tax, for example) is not sufficient to improve the quality of diets or prevent the associated health outcomes (NCDs). 1
Subsequent to South Africa’s implementation of SSB tax, a study was carried out to determine the feasibility of the tax strategy in seven sub-Saharan Africa, namely, Botswana, Namibia, Zambia, Uganda, Kenya, Tanzania and Rwanda. 4 Results of the three-year study indicated the strategy is feasible in all seven countries. However, countries other than Rwanda and Namibia have passed policies that promote the growth of the sugar industries for their economic growth that is in contradiction with the tax measures to decrease the consumption of sugar. 4
Since results indicate that the population in South Africa equivocates the SSB tax strategy by compensating their sugar through other sources or resorting to other obesity related foods 1, and some sub-Saharan countries have actively growing sugar industries, alternative solutions to combat obesity and NCDs need to be explored 4. It has been proposed that countries should pass a broader range of economic and legislative policies that aim to further decrease the consumption of sugar and ultra-processed foods, whilst increasing the demand for and access to healthier foods to be incorporated in diets. 1
However, legislative processes are not controllable by HCPs, nor can countries afford to wait for proposed legislations to take effect. It is therefore recommended that HCPs educate patients and communities in a holistic manner, as another strategy to combat high sugar intake related NCDs since it has tended to be more successful. 6,7
A holistic education approach to facilitate a multicomponent intervention is vital to ensure patients don’t compensate the loss of one bad habit, by adding another unhealthy habit as seen in the evidence above. 6 The following points offer a holistic educational approach to prevent obesity and its related NCDs:
- Patients should monitor and protect their mental and social well-being (through reduced screen time and healthy personal relationships) to improve behavioural skills that affect their diet. 6
- Patients should be made aware that the excessive intake of foods, snacks or beverages that are high in sugar, sodium, fat or are highly processed, leads to excessive amounts of energy- which leading to obesity and its related NCDs. 1,6,7
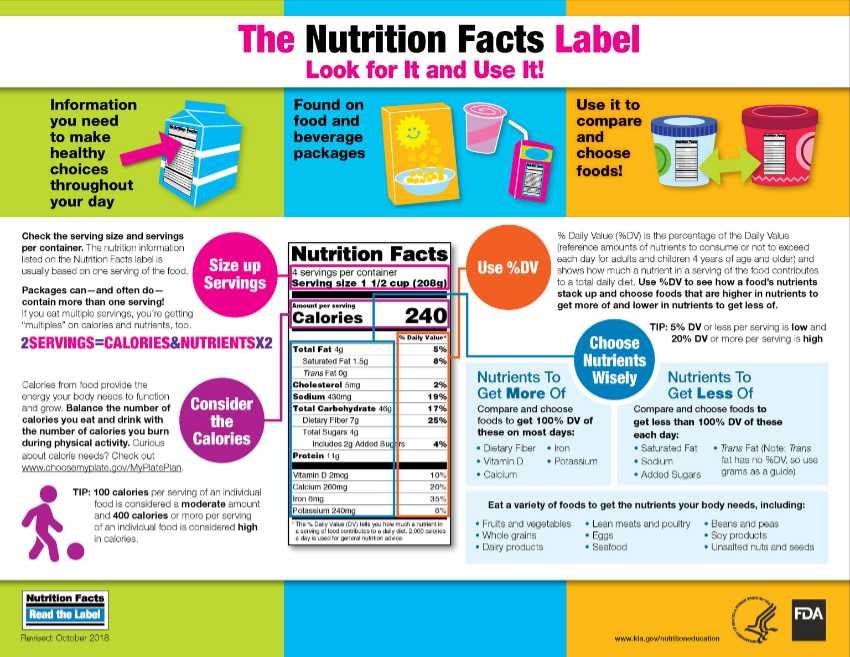
- Patients should be taught how to read food labels to make wiser diet choices. 8
- HCPs should promote increased levels of physical activity to patients in order to deplete stored energy, a key factor to obesity. 6
- The importance of a diet that is rich in a range of healthy foods and beverages should be taught to patients. 1,6
- HCPs should promote a higher consumption of fruits, vegetables, wholegrains, nuts, seeds, and adequate levels of animal sourced food will ensure that patients receive a lower but sustainable energy intake and provide micronutrients that unhealthy foods do not offer. 7
By empowering patients, all HCPs could assist patients to make better choices in their dietary lifestyle, to prevent obesity and related NDCs that are not only a sub-Saharan concern, but that of a worldwide concern. 1,6
A guide on how to read food labels 8 :
Referencing:
- Wrottesley, S.V., Stacey, N., Mukoma, G., Hofman, K.J. and Norris, S.A., 2021. Assessing sugar-sweetened beverage intakes, added sugar intakes and BMI before and after the implementation of a sugar-sweetened beverage tax in South Africa. Public Health Nutrition, 24(10), pp.2900-2910.
- Thow, A.M., Abdool Karim, S., Mukanu, M.M., Ahaibwe, G., Wanjohi, M., Gaogane, L., Amukugo, H.J., Ruhara, C.M., Ngoma, T., Asiki, G. and Erzse, A., 2021. The political economy of sugar-sweetened beverage taxation: an analysis from seven countries in sub-Saharan Africa. Global health action, 14(1), p.1909267.
- WHO. Fiscal Policies for diet and prevention of noncommunicable diseases. Geneva: World Health Organization; 2016. Technical meeting report (5–6 May 2015, Geneva, Switzerland).
- The Conversation: Academic Rigour, Journalistic Flair. 2019. We mapped the landscape for taxes on sugary drinks in seven African countries. https://theconversation.com/we-mapped-the-landscape-for-taxes-on-sugary-drinks-in-seven-african-countries-158243#:~:text=Over%2073%20countries%20had%20adopted,most%20of%20sub%2DSaharan%20Africa Date of access: 18 Feb. 2022.
- Marquez, P.V. and Farrington, J.L., 2013. The challenge of non-communicable diseases and road traffic injuries in sub-Saharan Africa: an overview.
- Lee, B.Y., Bartsch, S.M., Mui, Y., Haidari, L.A., Spiker, M.L. and Gittelsohn, J., 2017. A systems approach to obesity. Nutrition reviews, 75(suppl_1), pp.94-106.
- Hawkes, C., Ruel, M.T., Salm, L., Sinclair, B. and Branca, F., 2020. Double-duty actions: seizing programme and policy opportunities to address malnutrition in all its forms. The Lancet, 395(10218), pp.142-155.
- FDA. 2018. The nutrition facts label: look for it and use it! https://www.fda.gov/media/134412/download
- Ohri-Vachaspati, P., DeWeese, R.S., Acciai, F., DeLia, D., Tulloch, D., Tong, D., Lorts, C. and Yedidia, M.J., 2019. Healthy food access in low-income high-minority communities: a longitudinal assessment—2009–2017. International journal of environmental research and public health, 16(13), p.2354.
If you liked this post you may also like



